Robust and widespread antibody testing has emerged as a key strategy in the fight against SARS-CoV-2, the virus responsible for the COVID-19 pandemic. However current testing methods are too inaccurate or too expensive to be feasible on a global scale. But now, scientists at the Okinawa Institute of Science and Technology Graduate University (OIST) have developed a rapid, reliable, and low-cost antibody test.
The device, described in a proof-of-concept study published this week in Biosensors and Bioelectronics, uses portable lab-on-a-chip technology to accurately measure the concentration of antibodies present in diluted blood plasma.
Antibodies are proteins produced by the immune system to neutralize the virus. Research has found that COVID-19 antibodies are present in the later stages of infection and can linger in the blood after the infection has cleared, allowing previously infected individuals to be identified. Antibody tests are thus an important means of determining the full spread of the coronavirus -- information that is crucial to guide public health policies.
And yet many nations have so far failed to employ large-scale antibody testing.
"Many existing platforms for antibody tests are accurate and reliable, but they are costly and need to be carried out in a lab by trained operators. This means that it can take hours, or even days, to obtain results," said Dr. Riccardo Funari, first author and a postdoctoral researcher in the Micro/Bio/Nanofluidics Unit at OIST. "Other tests are easier to use, portable and rapid, but are not sufficiently accurate, which hampers testing efforts."
The researchers avoided this trade-off between accuracy and accessibility by developing an alternative antibody testing platform that combines powerful light-sensing technology with a microfluidic chip. The chip provides results within 30 minutes and is highly sensitive, detecting even the lowest clinically-relevant antibody concentration. Each chip is cheap to manufacture and negates the need for a lab or trained operators, increasing the feasibility of nation-wide testing.
And there's another distinctive advantage of this newly developed platform. "The test doesn't just detect whether the antibodies are present or absent -- it also provides information about the quantity of antibodies produced by the immune system. In other words, it's quantitative," said Professor Amy Shen, who leads the Micro/Bio/Nanofluidics Unit. "This greatly expands its potential applications, from treating COVID-19 to use in developing vaccines."
Illuminating the antibodies
The antibody testing platform consists of a microfluidic chip which is integrated with a fiber-optic light probe. The chip itself is made from a gold-covered glass slide with an embedded microfluidic channel. Using an electric voltage, the team fabricated tens of thousands of tiny spiky gold structures, each one smaller than the wavelength of light, on a glass slide.
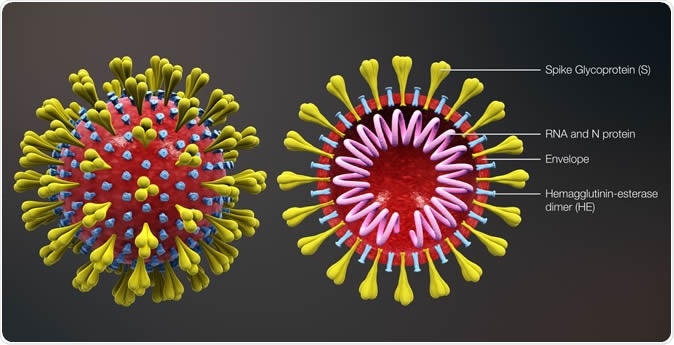
The researchers then modified these gold nanospikes by attaching a fragment of the SARS-CoV-2 spike protein. This protein is crucial for helping the coronavirus infect cells and causes a strong reaction from an infected person's immune system.
In this proof-of-concept study, the scientists demonstrated the principle behind how the test detects antibodies by using artificial human plasma sample spiked with COVID-19 antibodies that are specific to the spike protein.
Using a syringe pump, the sample is drawn through the chip. As the plasma flows past the protein-coated gold nanospikes, the antibodies bind to the spike protein fragments. This binding event is then detected by the fiber optic light probe.
"The detection principle is simple but powerful," said Dr. Funari. He explained that is it based on the unique behavior of electrons on the surface of the gold nanospikes, which oscillate together when hit by light. These resonating electrons are highly sensitive to changes in the surrounding environment, such as the binding of antibodies, which causes a shift in the wavelength of light absorbed by the nanospikes.
"The more antibodies that bind, the larger the shift in the wavelength of the absorbed light," added Dr. Funari. "The fiber optic probe is connected to a light detector which measures this shift. Using that information, we can determine the concentration of antibodies within the plasma sample."
A bright future
The large-scale roll-out of a quantitative test could greatly impact how COVID-19 is treated.
For example, quantitative tests could help doctors track how effectively a patient's immune system is fighting the virus. It could also be used to help identify suitable donors for a promising experimental treatment, called plasma transfusion therapy, where a recovered patient's antibody-rich blood is donated to currently infected patients to help them fight the virus.
Being able to measure the level of immune response can also aid vaccine development, allowing researchers to determine how effectively a trial vaccine triggers the immune system.
However, the researchers emphasized that the device is still undergoing active development. The unit aims to reduce the chip size to cut manufacturing costs and is also working on improving the reliability of the test.
"We have shown that the device works to detect different concentrations of the spike protein antibody in artificial human plasma samples. We now want to expand the test so that the chip can detect multiple different antibodies at the same time," said Dr. Funari. "Once the device is optimized, we plan to collaborate with local hospitals and medical institutions to perform tests on real patient samples."
Story Source:
Materials provided by Okinawa Institute of Science and Technology (OIST) Graduate University. Originally written by Dani Ellenby. Note: Content may be edited for style and length.
Journal Reference:
- Riccardo Funari, Kang-Yu Chu, Amy Q. Shen. Detection of antibodies against SARS-CoV-2 spike protein by gold nanospikes in an opto-microfluidic chip. Biosensors and Bioelectronics, 2020; 169: 112578 DOI: 10.1016/j.bios.2020.112578
Source:https://www.sciencedaily.com/releases/2020/09/200908131038.htm